Emergent Care / Stabilization: Start an intravenous (IV) line and evaluate for signs and symptoms of cardiac tamponade. If present and hemodynamically significant, drainage via pericardiocentesis or pericardial window should be performed as soon as possible.
Etiology / Pathophysiology: Pericarditis is an inflammation of the fibrous tissue sac surrounding the heart. The exact incidence of pericarditis is unknown, although data suggests it represents 5% of emergency department (ED) visits admitted for chest pain.
Pericarditis of an infectious etiology is predominantly viral (90%). The most common of these include coxsackievirus A or B, echovirus, Epstein-Barr virus, HIV, cytomegalovirus, and parvovirus B19. Viral pericarditis may also involve the myocardium, causing myopericarditis. SARS-CoV-2 is associated with both pericarditis and myocarditis with higher mortality than other viral illnesses. Additionally, rare cases of myocarditis following SARS-CoV-2 vaccination have been reported, predominantly in younger males.
The most common bacterial pathogens include Staphylococcus aureus, Streptococcus pneumoniae, and, in developing countries, tuberculosis. Fungi such as Candida spp and parasites such as Toxoplasma gondii also cause pericarditis.
Noninfectious causes include trauma, surgery (especially cardiothoracic surgery such as coronary artery bypass grafting), myocardial infarction, uremia, aortic dissection, myxedema, radiation, rheumatological conditions (including lupus, sarcoidosis, rheumatoid arthritis, and scleroderma), medications (including hydralazine, procainamide, methyldopa, phenytoin, and penicillin), and malignancy (eg, sarcoma, lymphoma, pericardial mesothelioma). Many cases are idiopathic.
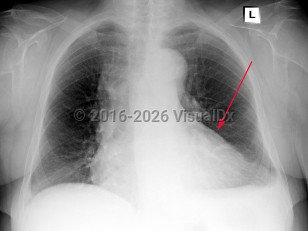
Symptoms and Signs: Acute pericarditis typically presents with sharp pleuritic chest pain, exacerbated by the supine position and improved with leaning forward. Fever and myalgias may be present but are not required features. On examination, a scratch-like friction rub (pericardial rub) may be heard, although this is present in less than 33% of cases. To make the diagnosis of pericarditis, the patient must have 2 of 4 criteria: pericardial rub, chest pain, ECG changes, and/or presence of a pericardial effusion. Chest pain has the highest incidence and is seen in 85%-90% of cases.
While not usually life-threatening, acute pericarditis can progress to cardiac tamponade or constrictive pericarditis in some complicated cases. Consider constrictive pericarditis in cases of unexplained heart failure. Tricuspid regurgitation is common in these patients and is associated with increased mortality. Other findings in constrictive pericarditis can include Kussmaul sign (a paradoxical increase in jugular venous pressure on inspiration), jugular venous distention, peripheral edema, hepatomegaly, and pericardial knock.
Predisposing Medical History and Risk Factors: As described above, viral infections often precede pericarditis, and patients may report systemic signs and symptoms of infection. Pericarditis should also be considered in any patient with recent cardiothoracic surgery or underlying rheumatologic disease. Recurrent pericarditis is seen in 15%-30% of patients.
Pericarditis
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
I31.9 – Disease of pericardium, unspecified
SNOMEDCT:
3238004 – Pericarditis
I31.9 – Disease of pericardium, unspecified
SNOMEDCT:
3238004 – Pericarditis
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
Drug Reaction Data
Subscription Required
References
Subscription Required
Last Reviewed:08/29/2022
Last Updated:02/12/2024
Last Updated:02/12/2024
Pericarditis