Polycystic ovary syndrome (PCOS) is a relatively common endocrine disorder, affecting 4%-6% of reproductive-aged women. It affects all races and ethnicities. PCOS is defined by chronic anovulation, hyperandrogenism, and often insulin resistance. The state of chronic anovulation leads to a polycystic appearance of one or both ovaries. Obesity is closely associated with PCOS and tends to exacerbate the pathophysiology of the syndrome; however, many women with PCOS are of a normal weight.
Although the exact etiology of the syndrome is unclear, women with PCOS have increased luteinizing hormone (LH) and low-to-normal follicle stimulating hormone (FSH). This is either a result of some inherent fault of hypothalamic-pituitary function, improper hypothalamic-pituitary-ovarian feedback mechanisms, or both. The increased LH stimulates an overproduction of androgens in the ovary; while some androgen will be converted to estrogen by aromatase, the overall hormonal milieu within the ovary is androgen dominant. This leads to an environment in which none of the smaller, immature ovarian follicles can arise as a mature dominant follicle. As such, the ovary takes on a polycystic appearance, with an overabundance of small follicles causing a cystic architecture on ultrasound.
Among women with PCOS, 50%-75% have clinically measurable insulin resistance. The exact cause of the insulin resistance is unclear and is likely multifactorial. It is known that high circulating levels of insulin increase ovarian androgen production and decrease hepatic sex hormone binding globulin, which leads to an overall increase in free androgens. Androgens increase insulin resistance, further progressing the disease.
Women with PCOS typically present with complaints of menstrual irregularity due to anovulatory abnormal uterine bleeding and/or difficulty conceiving. They are at increased risk of sexual dysfunction.
Over time, anovulation puts patients with PCOS at increased risk of endometrial cancer. The syndrome is also associated with a higher rate of cardiovascular disease and diabetes.
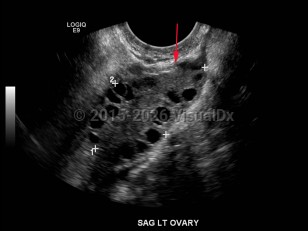
Polycystic ovarian syndrome
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
E28.2 – Polycystic ovarian syndrome
SNOMEDCT:
237055002 – Polycystic ovary syndrome
E28.2 – Polycystic ovarian syndrome
SNOMEDCT:
237055002 – Polycystic ovary syndrome
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:08/28/2018
Last Updated:09/25/2024
Last Updated:09/25/2024
Polycystic ovarian syndrome