Herpes simplex virus encephalitis, typically caused by herpes simplex virus type 1 (HSV-1), is characterized by the acute onset of fevers, headaches, and other neurologic signs and symptoms, including seizures, altered levels of consciousness, and personality changes. HSV encephalitis is the most common cause of sporadic fatal encephalitis in the United States and worldwide. Even with antiviral therapy, HSV encephalitis can result in significant morbidity and can even be fatal.
Infection with HSV leading to encephalitis can occur due to direct central nervous system (CNS) invasion via the trigeminal nerve or olfactory tract after HSV-1 oropharyngeal infection. This type of primary infection is common in patients under the age of 18. In patients over the age of 18, infection generally occurs either via CNS invasion following a recurrent episode of HSV-1 infection, or because of reactivation of latent HSV infection in the CNS without a primary or recurrent HSV-1 infectious process.
HSV encephalitis is not more common in immunosuppressed patients than in immunocompetent patients, although presentation can be atypical in immunosuppressed individuals. Immunosuppressed patients may present with more subacute symptoms that gradually develop over a long period of time, whereas immunocompetent hosts generally have a rapid onset of symptoms and, without intervention, progressive neurologic deterioration.
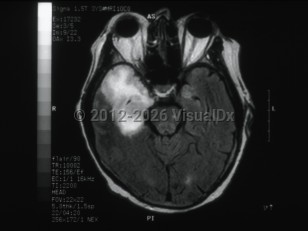
Clinically, patients typically present with focal neurologic signs that have been present for <1 week. In most cases of HSV encephalitis, the temporal lobe of the brain, usually unilateral, undergoes necrosis, and clinical findings reflect the areas of the brain that are affected. They include altered levels of consciousness, behavioral changes, focal cranial nerve deficits, ataxia, aphasia, and seizures. The majority of patients will also present with fever. The behavioral changes most commonly associated with HSV encephalitis are hypomania (including elevated mood, excessive animation, hypersexuality, and decreased sleep requirements), amnesia, and Klüver-Bucy syndrome, which is a behavioral syndrome that involves loss of typical anger and fear responses and increased sexuality. The Klüver-Bucy syndrome is thought to be associated with the proclivity of HSV encephalitis for the temporal lobes and limbic system structures. More rarely, HSV encephalitis can present as a brainstem syndrome and can result in the syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Special Considerations in Infants:
While most cases of HSV encephalitis that occur after the neonatal period are caused by HSV-1, HSV encephalitis in neonates is commonly due to HSV type 2 (HSV-2).
Potentially life-threatening emergency
Herpes simplex virus encephalitis
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
B00.4 – Herpesviral encephalitis
SNOMEDCT:
427796004 – Encephalitis due to human herpes simplex virus
B00.4 – Herpesviral encephalitis
SNOMEDCT:
427796004 – Encephalitis due to human herpes simplex virus
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Updated:05/26/2014
Potentially life-threatening emergency
Herpes simplex virus encephalitis