Intussusception is a telescoping or invagination of a part of the intestine into the lumen of an adjacent segment. Intussusception can present with variable severity. It can present with bowel ischemia and perforation with need for emergent surgical intervention, or it can present as relaxing / remitting abdominal pain of unclear etiology with intermittent symptoms and no signs of systemic illness. Jejunojejunal, jejunoileal, ileoileal, ileocolonic, and colocolonic are all types of intussusception that can occur, with the majority involving the small intestine.
Intussusception occurs in children and adults. It is the most common cause of bowel obstruction in children, where it presents with sudden onset of acute abdominal pain and inconsolability, and at times with emesis, a palpable abdominal mass, or hematochezia. Tucking knees into the torso is consoling in some instances. In pediatrics, intussusception is most commonly due to viral illnesses, with mesenteric lymphadenopathy creating a lead point to trigger intussusception. Tumors, polyps, Meckel diverticulum, or postsurgical adhesions are additional causes that can trigger intussusception.
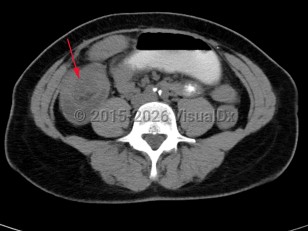
Intussusception in adults presents with similar symptoms: sudden-onset abdominal pain that can relax and remit, with or without symptoms of acute bowel obstruction and hematochezia. Intussusception in adults can also be caused by viral infections, polyps, or postsurgical adhesions, but there is greater concern for underlying malignancy – either small or large bowel or extrinsic (eg, lymphoma) – as a trigger point.
In both adults and children, prolonged intussusception can cause bowel ischemia, resulting in hematochezia due to mucosal sloughing and a risk of bowel perforation. Concern for intussusception should prompt emergent medical evaluation at a hospital with radiology, gastroenterology, and general surgery available on call.
Initial management requires ensuring hemodynamic stability, as many patients are dehydrated, and assessing concern for bowel perforation, which could require broad-spectrum antibiotics and urgent surgical intervention. Air or barium enemas can be both diagnostic and therapeutic. However, intussusception will frequently recur, in which case surgical resection is often required. Further imaging (ie, small bowel x-ray series, CT or MRI abdomen) can be utilized to identify the etiology if it is unknown based on presenting symptoms and a barium / air enema.
Potentially life-threatening emergency
Intussusception in Adult
Alerts and Notices
Important News & Links
Synopsis
Codes
ICD10CM:
K56.1 – Intussusception
SNOMEDCT:
49723003 – Intussusception of intestine
K56.1 – Intussusception
SNOMEDCT:
49723003 – Intussusception of intestine
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:09/25/2017
Last Updated:07/07/2024
Last Updated:07/07/2024
Potentially life-threatening emergency
Intussusception in Adult