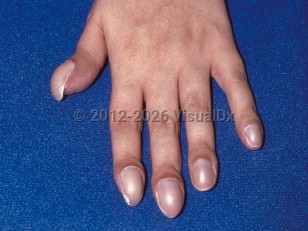
Clubbing, or acropachy, is an enlargement of the transverse and longitudinal curvature of the nails with hypertrophy of the soft tissues. It was first described by Hippocrates in the fifth century B.C. The etiology is unclear but may be related to increased vascularity of the fingers or vasodilation with subsequent increased blood flow to the fingers. Other proposed causes include tissue hypoxia, a neurocirculatory reflex, and genetic factors. Clubbing may involve both the fingers and the toes. Clubbing may be classified into 3 types: acquired, hereditary / congenital, and idiopathic.
The acquired form is the most common cause of clubbing, with cardiothoracic disorders (usually with associated hypoxia) accounting for 80% of cases. Pulmonary diseases are more common than cardiovascular disorders. Examples of thoracic organ disorders include bronchopulmonary diseases (eg, chronic and infective bronchiectasis, abscess and cyst of the lung, tuberculosis, sarcoidosis, pulmonary fibrosis, emphysema, chronic pulmonary venous congestion, asthma in infancy, pneumonia, Pneumocystis carinii pneumonia, and blastomycosis), thoracic tumors (eg, primary or metastatic bronchopulmonary cancers, pleural tumors, mediastinal tumors, Hodgkin disease, and lymphoma), and cardiovascular diseases (eg, congenital heart disease associated with cyanosis, thoracic vascular malformations, Osler-Weber-Rendu disease, congestive heart failure, subacute bacterial endocarditis, secondary polycythemia, myxoma, and Raynaud syndrome).
Gastrointestinal tract disorders account for 5% of cases of clubbing. Examples of gastrointestinal tract disorders include esophageal, gastric, and colon cancers; gastric leiomyosarcoma; diseases of the small intestine; colonic diseases (eg, amebiasis, ulcerative colitis, Crohn disease, familial polyposis, and Gardner syndrome); chronic active hepatitis; and primary or secondary cirrhosis. Endocrine system disorders (POEMS syndrome, Shwachman-Diamond syndrome, thyroid cancer) and hematological system disorders (primary / secondary polycythemia, hemoglobinopathies) may also account for some cases of clubbing. Other less common acquired causes of clubbing may include AIDS, opioid use disorder, hashish use disorder, alcohol use disorder, pregnancy, malnutrition, chronic mountain sickness (Monge disease), and lupus.
The hereditary / congenital form of clubbing may be of autosomal dominant inheritance with no associated systemic disease. This form is also more common in Black individuals and people of North African descent.
The presence of clubbing in only a few fingers may be idiopathic or secondary to local injury, whitlow, lymphangitis, subungual epidermoid inclusion, osteoid osteoma, enchondroma, gout, sarcoidosis, aneurysm of the aorta or the subclavian artery, subluxation of the shoulder, Pancoast tumor, and median nerve neuritis. If the clubbing is located in the feet, then the patient may have an abdominal aortic graft with sepsis.
Occupational exposure to vinyl chloride may cause clubbing. Poisoning by phosphorus, arsenic, alcohol, mercury, silica, and beryllium may cause clubbing.
Late-stage clubbing may result in hypertrophic osteoarthropathy and painful periosteal proliferation of long bones (eg, radius, ulna, tibia). Associated clinical findings include fever, arthralgia, or joint effusion. At times, there is cyanosis, hyperhidrosis, paresthesias, and muscular weakness.
The syndrome pachydermoperiostosis is characterized by hypertrophic osteoarthropathy and acromegaly. There is a hereditary form that is autosomal dominant with incomplete penetrance and is most severe in males. In the acquired form, there is no family history; it presents in older men and is associated with cardiopulmonary or gastrointestinal neoplasms or infections.
Transitory clubbing may occur physiologically in the newborn. Hereditary / congenital clubbing is present at birth. Otherwise, clubbing occurs gradually over a period of weeks to months.
Clubbing of nails - Nail and Distal Digit
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
R68.3 – Clubbing of fingers
SNOMEDCT:
4373005 – Clubbing of nail
R68.3 – Clubbing of fingers
SNOMEDCT:
4373005 – Clubbing of nail
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:06/18/2018
Last Updated:09/18/2025
Last Updated:09/18/2025
Clubbing of nails - Nail and Distal Digit