Staphylococcus aureus are aerobic gram-positive cocci that form clusters and short chains. They are responsible for a wide variety of diseases ranging from superficial skin and soft tissue infections to deep-seated and life-threatening infections with high morbidity and mortality rates, such as endocarditis and septicemia. In addition, S aureus is capable of secreting toxins that mediate illnesses like the toxic shock syndrome (TSS) and the staphylococcal scalded skin syndrome (SSSS).
S aureus is a ubiquitous colonizer of the skin and mucosal surfaces and can be found in the nares of 10%-40% of individuals in the community and in the hospital. Nasal carriage is also a source for the transmission of multiresistant staphylococci. Certain patient populations like dialysis patients, people with diabetes, people who use IV drugs, people with alcohol use disorder, and HIV-infected individuals are at a high risk for infections from staphylococci.
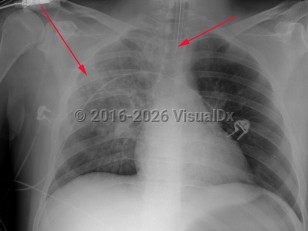
Staphylococcus aureus in responsible for about 1%-10% of community-acquired pneumonias and 20–30% of hospital-acquired pneumonias. Staphylococcus aureus pneumonia may result from air-borne contamination or aspiration or hematogenous seeding of the lungs from bacteremia or right-sided endocarditis. There may be a history of recent viral or influenzal illness. The clinical manifestations of staphylococcal pneumonia are similar to other causes of pneumonia except for a tendency to cause necrotizing infection with tissue destruction and cavitation. The patient will present with an abrupt onset of fever, tachypnea, pleuritic chest pain, and a productive cough with purulent sputum, which can be blood-tinged. Staphylococcus aureus is also one of the most common causes of empyema. In cases with accompanying endocarditis, stigmata-like subungual hemorrhages, murmur of aortic, tricuspid or mitral regurgitation, palmar Janeway lesions, and digital Osler nodes may be found.
Methicillin-resistant S aureus (MRSA) first emerged as an important nosocomial pathogen in the 1960s. In more recent years, community-acquired outbreaks of MRSA (CA-MRSA) have been described increasingly among healthy individuals lacking the traditional risk factors for staphylococcal infections.
A rapidly progressive necrotizing pneumonia in young, healthy adults and children has been described due to infection with strains of CA-MRSA containing the gene for the Panton-Valentine leucocidin (PVL), a toxin that induces lysis of host macrophages, thus impairing host response and facilitating tissue necrosis. The mortality from pneumonias caused by the PVL strains is very high.
Potentially life-threatening emergency
Staphylococcus aureus pneumonia - Pulmonary
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
J15.211 – Pneumonia due to Methicillin susceptible Staphylococcus aureus
SNOMEDCT:
441658007 – Pneumonia due to Staphylococcus aureus
J15.211 – Pneumonia due to Methicillin susceptible Staphylococcus aureus
SNOMEDCT:
441658007 – Pneumonia due to Staphylococcus aureus
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Updated:12/01/2020
Potentially life-threatening emergency
Staphylococcus aureus pneumonia - Pulmonary