Asymptomatic thoracic aortic aneurysm (TAA) patients can have cardiothoracic consultation for close outpatient follow-up or immediate bedside consultation for any other emergent concerns.
For aortic dissections and aortic rupture, the mainstays of treatment are:
- Impulse control (heart rate and blood pressure control).
- Transfusion if severely anemic.
- Reversal of anticoagulation.
- Pain control.
- Emergent cardiothoracic consultation.
Diagnosis Overview:
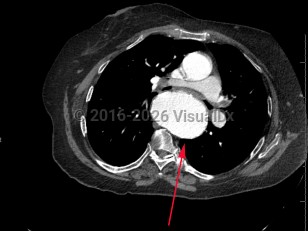
TAA is the dilatation of the artery compared to its original size; it is usually defined as the typical diameter of the artery increasing by 50%. A TAA will rarely manifest with symptoms, and about 95% of patients are asymptomatic. Catastrophic complications of TAA include aortic dissection and rupture, which are medical emergencies with high mortality rates. Most of these complications occur in the root or ascending aorta, followed by the descending aorta and aortic arch, respectively.
In the United States, about 13 000 patients die because of aortic disease each year, and TAA is the 18th most common cause of death among all individuals.
Risk factors include male sex, older age, history of hypertension, congenital heart defects (eg, bicuspid aortic valve), chronic obstructive pulmonary disease (COPD), coronary artery disease, smoking, previous aortic dissection, family history of aneurysmal disease, and genetic syndromes including Ehlers-Danlos, Loeys-Dietz, Marfan, and Turner syndromes. Historically, syphilis used to be the leading cause of TAA; however, with the use of antibiotics, the occurrence of syphilis-induced TAA has dropped dramatically.
Biochemical and mechanical forces lead to TAA causing wall weakness and expansion. Changes in aortic wall compliance lead to increased stress on the artery and during systolic impulse can further exacerbate wall fragility, leading to aneurysms. Several factors that can lead to rupture or dissection include but are not limited to aortic ulcers (disrupted atherosclerotic plaques), intimal atherosclerosis, and intramural hematomas. Infectious aortitis can cause pseudoaneurysms (false aneurysms that occur at the site of arterial injury from infection or trauma).
Management depends on the location, shape, and size of the aneurysm, as well as symptoms and concomitant cardiovascular disease. In asymptomatic patients, management may consist of blood pressure control, specifically with beta blockers for impulse control, surveillance, and patient education to watch for early signs and symptoms of complications. Following complete evaluation and risk assessment, surgical repair or replacement may be undertaken. Less than half of patients who have a ruptured TAA survive to the hospital. Mortality can be as high as 54% within 6 hours and 76% at 24 hours of rupture.
Related topic: cystic medial necrosis