Post-kala-azar dermal leishmaniasis (PKDL) is a mucocutaneous sequela of visceral leishmaniasis (VL). However, the condition may sometimes be seen in patients who have never had clinical VL.
VL, or kala-azar (meaning "black fever" in Hindi), is a systemic protozoal disease caused by parasites of the species Leishmania donovani and Leishmania infantum. The parasites exist in 2 forms: the amastigote form (in humans) and the promastigote form (in sandflies). The amastigote form is a round or oval structure that contains a nucleus and a DNA-containing body called the kinetoplast. The parasites are transmitted from infected sandflies to humans by sandfly bites. The majority of cases of VL are found in India, Bangladesh, Ethiopia, Sudan, South Sudan, Somalia, Kenya, Yemen, and Brazil.
PKDL is most prevalent in areas with endemic L donovani. Sporadic cases are reported in areas with endemic L infantum. Risk factors for the development of PKDL are not well known, but some studies have shown that previous treatment for VL with inadequate dosages of drugs, malnutrition, HIV infection, geographic area, and the age of the patient may play a role. A subset of patients who receive treatment for VL go on to develop PKDL months or years after treatment. However, for a substantial number of patients (10%-23%), there is no history of treatment.
The time lag between VL and PKDL differs in different parts of the world. In Sudan, PKDL lesions generally appear within 3-6 months of treatment in approximately 50%-60% of patients previously treated for VL. In contrast, PKDL in India manifests later (2-7 years after VL treatment), may persist for much longer (even up to 20 years), and develops in only about 5%-10% of patients treated for VL. Rarely, skin lesions may be noted with VL diagnosis, and the dermatologic presentation is diagnosed as para-kala-azar dermal leishmaniasis (paraKDL).
The pathogenesis of the disease is not clear, and why only a subset of patients develop PKDL is not known. It is thought that there is a shift from a Th2 response to a mixed Th1 / Th2 response following drug treatment or spontaneously. This leads to persistence of interleukin (IL)-10 in the blood and skin, which promotes persistence of infection.
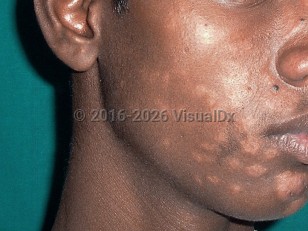
Post-kala-azar dermal leishmaniasis in Child
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
B55.0 – Visceral leishmaniasis
B55.1 – Cutaneous leishmaniasis
B55.9 – Leishmaniasis, unspecified
SNOMEDCT:
67896006 – Post-kala-azar dermal leishmaniasis
B55.0 – Visceral leishmaniasis
B55.1 – Cutaneous leishmaniasis
B55.9 – Leishmaniasis, unspecified
SNOMEDCT:
67896006 – Post-kala-azar dermal leishmaniasis
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:01/21/2024
Last Updated:01/31/2024
Last Updated:01/31/2024
Post-kala-azar dermal leishmaniasis in Child