Bladder calculi, or cystoliths, once a common cause of urologic pathology, have become increasingly rare in the United States over the last few decades. This condition is distinct from nephrolithiasis or kidney stones, which are now much more common than bladder calculi.
The decreased incidence of bladder calculi is largely because the 2 conditions principally associated with bladder stones, urinary stasis (most commonly due to benign prostatic hyperplasia [BPH]) and urinary tract infections (UTIs), are now more easily and frequently treated. BPH, once only effectively treated with surgery, is now frequently effectively and more easily treated with a combination of alpha blockers, 5-alpha reductase inhibitors, or transurethral resection. Consequently, the number of men suffering from chronic urinary retention has significantly decreased. Urinary stasis in the setting of neurogenic bladder is also a common etiology of bladder stone formation.
When urine is chronically retained in the bladder, any nidus, such as a small fragment of a stone passed from the ureter, a bladder diverticulum, or a foreign body such as a ureteral stent or Foley catheter, can serve as a site for the precipitation and deposition of uric acid. In most retrospective studies of bladder stone composition, nearly all stones (as many as 80%) are entirely composed of uric acid, and most of the remainder contain a substantial portion of uric acid. Interestingly, neither gout or hyperuricemia appear to be contributory factors in the formation of bladder calculi. This is qualitatively different than nephrolithiasis, which in the United States is primarily due to calcium oxalate or calcium phosphate stones.
Infrequently, stones may be formed from calcium oxalate, calcium phosphate, ammonium urate, cystine, or struvite (calcium-ammonium-magnesium phosphate or "triple phosphate"). Stones composed of struvite are almost always associated with chronic UTI and colonization with Proteus. An additional provoking factor in bladder stone formation is thought to be any condition that causes urothelial inflammation such as UTI and bacteriuria or urothelial dysplasia.
Demographically, patients with bladder stones are most frequently men over the age of 45, although patients with neurogenic bladder frequently develop stones at any age.
Bladder stones, particularly large and nonobstructive stones, do not frequently cause symptoms. Larger stones are thought to be less able to move significantly within the bladder and cause injury to the bladder wall and seem to be less prone to lodge in the bladder infundibulum / neck and cause acute obstruction. When patients do present with symptoms, they may be nonspecific and include suprapubic discomfort, hematuria, dysuria, urinary frequency, urinary hesitancy or poor urine stream, penile pain in male patients, or cloudy urine.
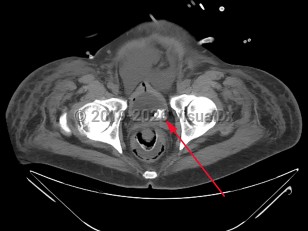
Urinary bladder calculus
Alerts and Notices
Important News & Links
Synopsis
Codes
ICD10CM:
N21.0 – Calculus in bladder
SNOMEDCT:
70650003 – Urinary bladder stone
N21.0 – Calculus in bladder
SNOMEDCT:
70650003 – Urinary bladder stone
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
Drug Reaction Data
Subscription Required
References
Subscription Required
Last Reviewed:08/16/2018
Last Updated:01/23/2025
Last Updated:01/23/2025
 Patient Information for Urinary bladder calculus
Patient Information for Urinary bladder calculus
Premium Feature
VisualDx Patient Handouts
Available in the Elite package
- Improve treatment compliance
- Reduce after-hours questions
- Increase patient engagement and satisfaction
- Written in clear, easy-to-understand language. No confusing jargon.
- Available in English and Spanish
- Print out or email directly to your patient
Upgrade Today

Urinary bladder calculus